Washington, DC – Today, the House voted on a package of legislation to address the opioid crisis, while at the same time Republicans at all levels have doubled down on their attacks on people with pre-existing conditions, including opioid use disorder, in the courts, through legislation and through regulations that promote junk plans and restrict Medicaid. In response, Leslie Dach, chair of Protect Our Care, issued the following statement:
“It’s past time that Republicans do the things that would truly support the families suffering from this crisis: end its assault on Medicaid, upon which four in 10 Americans with opioid use disorder relies, and back down from its constant attacks on people people with pre-existing conditions.”
ADDITIONAL BACKGROUND: How Republican Health Care Sabotage Is Exacerbating The Opioid Crisis
BY THE NUMBERS
- More than half of people with an opioid use disorder earn incomes below 200 percent of the federal poverty line.
- In 2014, Medicaid paid for 25 percent of all addiction treatment nationwide.
- It is estimated that Medicaid expansion covers four in 10 people with an opioid use disorder.
- The opioid epidemic is now the most deadly drug overdose crisis in U.S. history. In 2016, roughly 64,000 Americans died of drug overdoses, meaning that more American lives were lost due to drug overdoses in 2016 than were lost in combat during the entirety of the Vietnam War. Two-thirds of 2016 drug overdoses involved opioids.
- Medicaid expansion has reduced unmet need for substance use treatment by more than 18 percent. Recent research finds that Medicaid expanding reduced the unmet need for substance use treatment by 18.3 percent.
HOW PRESIDENT TRUMP & CONGRESSIONAL REPUBLICANS ARE WORKING TO DISMANTLE MEDICAID
- President Trump and his Republican allies in Congress have repeatedly tried to slash Medicaid funding, including by imposing per-capita caps. Last year, the House of Representatives passed the American Health Care Act (AHCA), which included a per-capita limit on federal Medicaid spending and would have resulted in huge cuts to Medicaid across states. After failing to pass the AHCA in the Senate, Republicans have relentlessly continued their attacks on Medicaid. In December, the Trump Administration went so far as to propose a budget that called for $1.4 trillion in cuts to Medicaid.
- The Trump Administration is now encouraging new hurdles for Medicaid enrollees in order to keep their coverage. Experts warn that work requirements are fundamentally bureaucratic hurdles designed to restrict access to health care rather than increase employment. Previous examples show that requiring enrollees verify their employment or work-related activities reduces enrollment among those still eligible for Medicaid.
- President Trump and Congressional Republicans are targeting Medicaid to pay for tax cuts to the wealthy. Last December, President Trump signed a $1.5 trillion tax bill that disproportionately benefits the wealthy. How do Republicans plan on paying for it? Speaker Ryan’s answer is clear: “Frankly, it’s the health care entitlements that are the big drivers of our debt.” Republicans’ approach is simple: cut programs like Medicaid that support working families.
- Restricting access to Medicaid threatens lives and impedes states’ ability to respond to the opioid epidemic. Four in ten Americans with an opioid use disorder relies on Medicaid for access to treatment, and in cases of overdose, for life-saving overdose reversal medication. By cutting funding to Medicaid and restricting the eligibility of those who can enroll, the Trump Administration is people’s lives at risk and is depriving states of funding and resources they depend on to fight the opioid epidemic.
BY HELPING PEOPLE ACCESS TREATMENT AND OVERDOSE-REVERSAL MEDICATION, MEDICAID SAVES LIVES
In 2014, Medicaid Paid For 25 Percent Of Spending For Addiction Treatment. “A 2014 study by Truven Health Analytics researchers found that Medicaid paid for about 25 percent — $7.9 billion of $31.3 billion — of projected public and private spending for addiction treatment in 2014. That made it the second-biggest payer of addiction treatment after all local and state government programs.” [Vox, 2/13/18]
By Expanding Access To Naloxone, Medicaid Has Saved Lives. “We estimate that in Massachusetts 868 opioid-related deaths were averted in 2016 (13 per 100,000 population). By contrast in Tennessee, which did not expand its Medicaid program, only 11 opioid-related deaths were averted in 2016 (0.17 per 100,000 population). Both states have been hit particularly hard by the opioid epidemic: Opioid-related deaths in 2015 were 20.9 and 21.5 per 100,000 in Massachusetts and Tennessee, respectively.” [Commonwealth Fund, 7/5/17]
[Commonwealth Fund, 7/5/17]
MEDICAID EXPANSION HAS INCREASED ACCESS TO TREATMENT
Medicaid Helps Make Buprenorphine And Naloxone, Drugs Used To Treat Opioid Use Disorder, Affordable. “These data are consistent with other evidence that Medicaid expansion is improving access to care for people with opioid use and other substance use disorders. Medicaid makes medications like buprenorphine and naloxone, which are prescribed to combat opioid use disorders, affordable for beneficiaries.“ [Center on Budget and Policy Priorities, 2/28/18]
Medicaid Expansion Has Improved Access To Substance Treatment Services. “Evidence also suggests that Medicaid expansion improved access to substance use treatment services more broadly. After expanding Medicaid, Kentucky experienced a 700 percent increase in Medicaid beneficiaries using substance use treatment services. Use of treatment services rose nationally as well; one study found that expanding Medicaid reduced the unmet need for substance use treatment by 18.3 percent.” [Center on Budget and Policy Priorities, 2/28/18]
In Ohio, Medicaid Has Helped Those With Substance Use Disorders Access Mental Health Services. “An Ohio study found that 59 percent of people with opioid-use disorders who had gained Medicaid coverage under expansion reported improved access to mental health care. Nationwide, the share of people forgoing mental health care due to cost fell by about one-third as the ACA, including Medicaid expansion, took effect.” [Center on Budget and Policy Priorities, 2/28/18]
MEDICAID GIVES STATES MORE RESOURCES TO ADDRESS THE OPIOID EPIDEMIC
Medicaid Is A Sustainable Source Of Funding Compared To Short-Term Grants. “Now that more people with SUDs are eligible for Medicaid, states can significantly improve treatment for people with SUDs by improving Medicaid-covered services. Medicaid can be a sustainable funding source for providers, as opposed to capped, short-term grant funding.” [Center on Budget and Policy Priorities, 2/28/18]
There Is No Substitute For Comprehensive Health Care In Fighting The Opioid Epidemic. In response to the opioid epidemic, Republicans proposed creating a $45 billion fund. However, as the Center for American Progress analyzes, “The Senate opioid fund is no substitute for comprehensive health coverage.” Why? Because “Even if the entirety of the fund were available to cover low-income individuals being treated for OUD, $45 billion would provide only half of the $91 billion that would be available under the ACA for health coverage alone.” [Center for American Progress, 6/20/17]
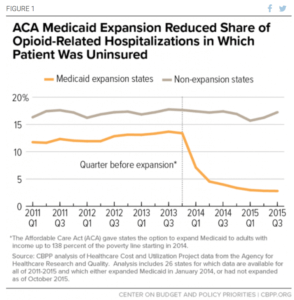
Thanks To Medicaid Expansion, The Uninsured Rate For Opioid-Related Hospitalizations Dropped In Expansion States. “In Medicaid expansion states, the uninsured rate for opioid-related hospitalizations plummeted by 79 percent, from 13.4 percent in 2013 (the year before expansion implementation) to 2.9 percent in 2015. The decline in non-expansion states was a much more modest 5 percent, from 17.3 percent in 2013 to 16.4 percent in 2015.” [Center on Budget and Policy Priorities, 2/28/18]
[Center on Budget and Policy Priorities, 2/28/18]
PUBLIC HEALTH, LAW ENFORCEMENT EXPERTS AGREE: MEDICAID IS KEY TOOL IN OPIOID FIGHT
A Panel Of Public Health Officials, Policy Experts, And Law Enforcement Officials Found Medicaid Among Most Important Programs In Combating Opioid Epidemic. Investing in Medicaid was the third most cited response when a panel of thirty experts were asked where they would put money to combat the opioid epidemic. [New York Times, 2/14/18]
Jay Unick, University Professor: Medicaid Expansion Is Most Important Intervention To Improve Opioid Epidemic. Medicaid expansion would be “the most important intervention for improving outcomes related to the opiate epidemic…all the other interventions discussed here only work if individuals have access to quality health care.” [New York Times, 2/14/18]
160 National, State, and Local Organizations Warn That Trump’s Medicaid Sabotage Will Hurt Those With Substance Use Disorders in Letter to Secretary Azar: “CMS’s Medicaid work requirements policy is directly at odds with bipartisan efforts to curb the opioid crisis…and will have a significant and disproportionately harmful effect on individuals with chronic health conditions, especially those struggling with substance use disorders (SUDs) and mental health disorders.” [Letter, 2/15/18]
Signatories include: ADAP Advocacy Association (aaa+); Addiction Policy Forum, Advocacy Center of Louisiana; AIDS United, Alameda County Community Food Bank; American Association on Health and Disability; American Association of People with Disabilities; American Association for the Treatment of Opioid Dependence (AATOD); American Civil Liberties Union; American Federation of State; County & Municipal Employees (AFSCME); American Foundation for Suicide Prevention; American Group Psychotherapy Association; American Psychological Association; American Society of Addiction Medicine; Association for Ambulatory Behavioral Healthcare; Bailey House, Inc.; Board for Certification of Nutrition Specialists; Brooklyn Defender Services; CADA of Northwest Louisiana; California Consortium of Addiction Programs & Professionals; California Hepatitis Alliance; Caring Across Generations; Caring Ambassadors Program; CASES; Center for Civil Justice; Center for Employment Opportunities (CEO); Center for Health Law and Policy Innovation; Center for Law and Social Policy (CLASP); Center for Medicare Advocacy; Center for Public Representation; Charlotte Center for Legal Advocacy; CHOW Project; Coalition of Medication Assisted Treatment Providers and Advocates; Colorado Center on Law and Policy; Community Access National Network (CANN); Community Catalyst; Community Health Councils; Community Legal Services of Philadelphia; Community Oriented Correctional Health Services; Community Service Society; Connecticut Legal Services; Consumer Health First; C.O.R.E. Medical Clinic, Inc.; Council on Social Work Education; CURE (Citizens United for Rehabilitation of Errants); DC Coalition Against Domestic Violence; Desert AIDS Project; Disability Rights Arkansas; Disability Rights Wisconsin; Drug Policy Alliance; EAC Network (Empower Assist Care); EverThrive Illinois; Facing Addiction with NCADD; Faces & Voices of Recovery; FedCURE; First Focus; Florida Health Justice Project, Inc.; Food & Friends; The Fortune Society; Forward Justice; Friends of Recovery – New York; Futures Without Violence; God’s Love We Deliver; Greater Hartford Legal Aid; Greenburger Center for Social and Criminal Justice; Harm Reduction Coalition; Health Law Advocates; Hep Free Hawaii; Hepatitis C Support Project/HCV Advocate; Heartland Alliance; HIV Medicine Association; Horizon Health Services; Hunger Free America; ICCA; Illinois Association of Behavioral Health; The Joy Bus; JustLeadershipUSA; Katal Center for Health, Equity, and Justice; The Kennedy Forum; Kentucky Equal Justice Center ; Kitchen Angels ; Justice in Aging ; Justice Consultants, LLC; Lakeshore Foundation; Law Foundation of Silicon Valley; Legal Action Center; The Legal Aid Society; Legal Council for Health Justice; Life Foundation; Live4Lali; Liver Health Connection; Maine Equal Justice Partners; MANNA (Metropolitan Area Neighborhood Nutrition Alliance); Massachusetts Law Reform Institute; McShin Foundation; Mental Health America; Mental Health Association in New York State, Inc. (MHANYS); Michigan Poverty Law Program; Minnesota Recovery Connection; Mississippi Center for Justice; NAACP; The National Alliance to Advance Adolescent Health; National Alliance on Mental Illness; NAMI-NYS; National Alliance of State & Territorial AIDS Directors; National Association of Addiction Treatment Providers; National Association of County Behavioral Health & Developmental Disability Directors; National Association for Rural Mental Health; National Association of Social Workers; National Center for Law and Economic Justice; National Coalition Against Domestic Violence; National Council on Alcoholism and Drug Dependence, Phoenix; National Council for Behavioral Health; National Council of Churches; National Disability Rights Network; National Employment Law Project; National Federation of Families for Children’s Mental Health; National Health Care for the Homeless Council; National Health Law Program; National HIRE Network; National Juvenile Justice Network; National LGBTQ Task Force; National Low Income Housing Coalition; National Organization for Women; The National Viral Hepatitis Roundtable; NC Justice Center; New Haven Legal Assistance Association; New York Association of Alcoholism and Substance Abuse; New York Association of Psychiatric Rehabilitation Services; New York Lawyers for the Public Interest; New York State Council for Community Behavioral Healthcare; Open Hands Legal Services; Osborne Association; Outreach Development Corp.; The Partnership for Drug Free Kids; PICO National Network; The Poverello Center, Inc.; Project Inform; Public Justice Center; Root & Rebound; Ryan White Medical Providers Coalition; Safer Foundation; Sargent Shriver National Center on Poverty Law; School Social Work Association of America; Sea Island Action Network, South Carolina; The Sentencing Project; Shatterproof; Society of General Internal Medicine; Southern Center for Human Rights; Southern Poverty Law Center; Students for Sensible Drug Policy; TASC of the Capital District, Inc.; Tennessee Justice Center; Three Square Food Bank; Transitions Clinic Network; Treatment Action Group; Treatment Alternatives for Safe Communities (TASC) – Illinois; Treatment Communities of America; Virginia Poverty Law Center; Western Center on Law & Poverty